The Amma Resonance Healing Foundation – Peter Chappell’s legacy for Africa
By Harry van der Zee, MD
Introduction
This article is in honor of the late Peter Chappell (1941-2023) and gives testimony to the huge impact his creative and unconventional mind had and will continue to have on the lives of literally millions of people. While this impact may become world-wide, the focus in this article is especially on the projects in Africa.
The medical establishment and media have a strong bias towards homeopathy and its terminology. This fact is a serious hindrance in making the amazing technology and method that Peter developed available to as many people as possible. In order to cross that bridge of scepticism and disbelief we have therefore started to use more widely accepted scientific language to explain the work we do. Besides that we focus on data collection and clinical studies whenever there is an opportunity for it. In this article both aspects will be covered.

Photo: Peter Chappell in Devon, where he lived for the last decade of his life. (Photo: Harry van der Zee, 2014)
How it started
Around the turn of the century, Africa faced a devastating AIDS epidemic. Entire villages were wiped out, with young adults being particularly affected, resulting in millions of AIDS orphans.
While AIDS drugs were widely available in the West, Africans were deprived of any treatment, leading to thousands of deaths. In 2001, UK homeopath Peter Chappell travelled to Ethiopia to explore whether homeopathy could offer a solution for the estimated 25 million Africans suffering from HIV/AIDS. Due to the scarcity of homeopaths in Africa, there was a need for a remedy that any doctor or nurse could prescribe with consistent results.
Using the homeopathic principle of resonance, Peter discovered a new method to create a remedy based on the genus epidemicus of an epidemic disease. This method became known as PC Technology, an advancement in homeopathy or, to avoid that biased term, Information Medicine. The first remedy, PC1, was used in thousands of cases with very positive results, confirmed by research.
ARHF
The foundation of ARHF stems from the remarkable success of resonance-based remedies (PC Remedies) in treating AIDS, malaria, and other epidemic diseases in Africa. With a primary focus on combating epidemics – especially in sub-Saharan Africa, where millions are affected and medical aid is often scarce – ARHF offers a vital alternative. Pharmaceutical drugs, when available, frequently cause side effects or lose effectiveness due to resistance.
After witnessing and publishing the impressive results of PC1 in Malawi, Dutch homeopaths Corrie Hiwat and Harry van der Zee partnered with Peter Chappell to establish ARHF and advance his ground-breaking work.
Based in the Netherlands, ARHF is a non-profit organisation committed to making a difference. Services are provided free of charge or, when possible, at cost price or below. All board members and contributors, located across the globe, work in an honorary capacity to further the organisation’s mission.
Recognized by the Dutch Tax Administration as a ‘Public Benefit Organization’ (ANBI status), ARHF is dedicated to improving health outcomes in some of the world's most underserved regions.
Mission
ARHF is dedicated to fostering health, wellbeing, and the alleviation of suffering on both individual and collective levels. Embodying the universal values of compassion, care, and generosity, the term 'Amma' symbolises these principles, resonating across diverse cultures worldwide. ARHF's primary focus lies within the African continent. ARHF promotes the development of healing through resonance to boost the immune system by inducing a self-healing response in individuals. This approach is aimed at the treatment and prevention of disease.
Vision
In homeopathy, human beings are perceived as holistic entities where physical, emotional, mental, and spiritual facets intricately intertwine to form an indivisible whole.
Symptoms and ailments are manifestations of an organism's innate drive towards wholeness and growth. Central to this understanding is the acknowledgment of the body's inherent self-healing capabilities, wherein symptoms serve as meaningful indicators of imbalance.
Healthcare interventions should bolster individuals' inherent capacity for self-resolution and preserve their holistic integrity. By addressing collective health challenges such as epidemics, trauma, and lifestyle diseases, ARHF endeavours to optimise both individual and societal wellbeing.
Goal
ARHF's overarching goal is to democratise access to its interventions, ensuring that those most in need can benefit from improved health outcomes. By prioritising conditions and regions where interventions yield the greatest impact, ARHF seeks to foster positive transformation on both individual and community levels, with a current focus on Africa.
Embodying the principle of self-reliance, ARHF operates through networks of volunteers, particularly in rural areas, to effectively address health challenges. Local teams, under the umbrella of Amma4Africa, autonomously manage projects, supported by ARHF through training and resources. These decentralised efforts are coordinated through the Africa Heart Team, serving as a pivotal link between the ARHF Heart Team and Board and grassroots initiatives.
ARHF's initiatives are further bolstered by partnerships with licensed European pharmacies (Helios Pharmacy, Hahnemann Apotheek and Apotheke z. heiligen Florian) for the production of Source Remedies (PC Remedies) and by a Source Work Team that provides Source Audios. [PC Remedies can only be ordered by a code number, as indications are not allowed on a label; Helios uses SR, the other pharmacies PC; e.g. PC158n/SR158n for diabetes type 2.]
Method
Leveraging the concept of vital energy and the principles of coherence, ARHF endeavours to restore balance and vitality by delivering targeted ‘coherence-inducing information’. This innovative approach, encompassing water-based and sound-based interventions, harnesses the inherent healing potential within individuals.
Making sense of Information Medicine
Introduction
Think about how people used aspirin for centuries without really knowing how it worked in the body. Similarly, we've lived on Earth, dealing with gravity's pull, without fully understanding it. The same holds true for the origin of life, as chemistry can’t explain the creation of the complex molecules needed for living organisms to emerge. But now, a new field called Information Medicine is challenging old ideas and bringing together modern science with ancient healing traditions. Let's break it down.
Understanding Information Medicine
Information Medicine is all about finding connections between traditional healing practices and modern science. At its core is the idea of a Life Force or Vital Energy that flows through all living things, influencing our health. To explain this scientifically, we look at concepts from thermodynamics (the study of heat and energy), quantum physics, water memory, and how information is stored and transmitted.
Thermodynamics and quantum biology
In the world of life and energy, thermodynamics and quantum biology intersect in fascinating ways. Thermodynamics helps us understand how life strives for maintaining harmony in living organisms that are continuously undergoing change. Any serious disruption (increased entropy – state of disorder – in terms of thermodynamics) causes disharmony and can lead to illness. Quantum biology reveals that coherence is a key quantum phenomenon supporting life dynamics. To restore balance and to create coherence, the body needs to receive what we can call coherence inducing information. Organisms are dissipative systems and the export of entropy is a key element in keeping the system functional. [1,2]
Water memory and information retention
Coherent domains are groups of water molecules that act together in a quantum-coherent state, essentially behaving as a single entity rather than as individual molecules. These coherent domains play a critical role in biological processes, particularly in the formation and functioning of proteins and DNA. Therefore, water isn't just a simple liquid. 99% of all molecules in the human body are water molecules. Studies suggest that water can remember information and convey it to a living being, challenging our traditional views of memory storage. Water's structure can also be influenced by electromagnetic fields, sound and light. [3,4,5]
Putting it all together
When we combine ideas from thermodynamics, quantum biology, and water memory, we get a clearer picture of how Information Medicine can be used to promote health and wellbeing. From the tiniest quantum levels to our overall health, these disciplines show us the intricate balance between order and disorder, health, and disease.
Using sound for healing
Sound therapy, based on resonance and frequency, has a long history of promoting relaxation and wellbeing. Encoding information in sound is a new development in Information Medicine. Just like water imprinted with information, encoded sound can improve harmony through export of entropy (a degree of disorder/chaos) and optimise health. [6,7]
Putting theory into practice
The current materialistic paradigm to understand the phenomena of life is widely insufficient. We do not understand life in its details. In using Information Medicine, clinical observation has the potential to conceptualise life in a more coherent manner despite many open questions. Remedies tailored to specific conditions aim to restore balance and kickstart the body's own healing mechanisms. Clinical observation shows the full expression of the syndromes treated and the organism’s potential for healing, as also the effectiveness and safety of Information Medicine.
Conclusion
Information Medicine blends ancient wisdom with modern science, offering a new way to understand and promote health and explore human potential. By combining principles from various fields, a framework can be provided for better understanding of living systems and its properties as well as improving our wellbeing. As research in this area continues, Information Medicine holds the promise of transforming healthcare with personalised, non-invasive interventions.
How PC technology works
‘The future of medicine will be the medicine of frequencies’ — Albert Einstein
‘If there is magic on this planet, it is contained in water’ — Loren Eiseley
The clinical results of using PC technology for various conditions are objectively observable and highly convincing [8-15]. For patients, this effectiveness is crucial, but the inquisitive mind seeks to understand how healing can occur without using any chemical substances.
Modern research into water provides a basis for understanding the mechanisms behind PC remedies. Water is essential for all living beings. About two-thirds of the human body is water, but if we look at the molecular level, 99% of all molecules in our bodies are water molecules. These water molecules are not just passive carriers; they actively participate in life's processes.
Water is a fascinating substance with an important recently discovered characteristic: it can store and memorise information. Besides the known three phases of water – gas, liquid, and solid – researchers have found evidence for a fourth phase at interfaces, called exclusion-zone (EZ) water. Much of the water in cells is near hydrophilic (literally ‘water loving’) surfaces and thus ordered in a structured lattice, similar to a liquid crystal. This ordered state allows water to store information because modifications in the positions of oxygen and hydrogen atoms within this lattice constitute data. The potential for high-density information storage in water is extraordinary, given the various oxidation states of oxygen atoms. Information can be transmitted to the body via imprinted water or frequencies – electromagnetic waves of sound or light. [6, 16-17].
Information Medicine and PC technology leverage water's ability to receive and store information to regulate cell behaviour [18-19]. PC remedies are created by embedding water or sound with information related to specific conditions or diseases, based on all known signs and symptoms of that condition. Resonance occurs when the frequency of an external source matches the frequency of a system, leading to an amplification of energy. Small amounts of energy or information can have large effects on the body by resonating with the natural frequencies of the coherent domains in water.
Coherence, a key quantum phenomenon, supports life dynamics. Disease and disharmony result from increased entropy (chaos). To restore balance and create coherence in a diseased organism, the body needs coherence-inducing information. PC remedies provide this information as they are imprinted with the necessary data for the body to overcome or prevent disease [2, 4, 7, 20].
For explaining how the body stores and utilizes this information for healing, the fourth phase of water is a promising candidate.
Some of the main aims of ARHF
AIDS in Africa
In the 1980s, the first AIDS patients were diagnosed. Soon it was discovered that the Acquired Immune Deficiency Syndrome (AIDS) was caused by a virus called HIV. With the immune system destroyed by the HIV infection, patients lost their ability to fight other infectious diseases and ultimately died. Since the beginning of the HIV/AIDS epidemic approximately 42.3 million people have died from HIV-related causes globally (WHO 2024), of which ±25 million in sub-Saharan Africa.
In Africa, HIV/AIDS spreads among men and women alike, whereas in many other parts of the world, infections occurred predominantly in homosexuals and drug addicts. Certain aspects of African sexual practices significantly facilitate the spread of HIV/AIDS in the heterosexual population: gender roles, unsafe sex practices, poverty driven prostitution and rape. Unawareness of the disease and taboo also play an important role, especially in the early years.
The high mortality rate in sub-Saharan Africa is also due to limited access to healthcare, late diagnosis, and insufficient availability of anti-retroviral therapy (ART). Despite the increasing use of anti-retroviral drugs (ARVs) in recent years, many more AIDS deaths are predicted in sub-Saharan Africa in the coming years. Therapy resistance is a growing problem, and many children born with HIV no longer respond to ARVs, facing an early death.
In 2001, when Peter Chappell went to Ethiopia, there was essentially no treatment available for HIV/AIDS in Africa. After documenting around 70 cases of AIDS patients in Ethiopia, he compiled all their AIDS-related symptoms and sought a homeopathic remedy that would match the disease. To his disappointment, no such remedy was known. Having an inquisitive mind and a background of years of being a research and development engineer, Peter then explored the possibility of creating an HIV/AIDS specific remedy himself.
In 2002, he succeeded and created a remedy he later named PC1. Using PC technology he imprinted the symptom totality of AIDS in Africa directly in water. As the remedy contains no potentially harmful substances, PC1 can be safely prescribed to all infected and in all phases of the disease, without any side effects. To Peter’s great joy, he found that all patients who had the remedy responded well to it. Their energy levels and appetites quickly returned to normal, and their pains and lung problems subsided. They soon resumed normal, active lives. [11]
Since 2002, PC1 has been used in many African countries by doctors, nurses, and community health workers trained by ARHF. Their reported results were similar to those initially observed by Peter Chappell. In several studies, clinical observations confirmed that AIDS patients taking PC1 recover from their AIDS-related symptoms rapidly. The significant decrease in opportunistic infections indicated a restoration of their immune system, confirmed by rising CD4 counts and reduced viral loads. [9, 10, 12, 15, 21-22]

Happy face in Burundi after treatment (Photo Gerda Hofstra, 2013)
Aids research
For doctors and nurses active in the field, directly experiencing clinical feedback from observing their patients is sufficient for using PC remedies with confidence. Meanwhile, to promote the treatment and prevention programmes and make them available to increasing numbers of people, gathering data and conducting research is a priority for ARHF. Often, however, the facilities for research in the field are lacking, making it challenging to conduct studies in the mostly rural settings where Amma4Africa teams are active.
Below is a summary of some of the data gathered and research conducted.
Ever since PC1 for HIV/AIDS was first used in Africa in 2002, consistent positive clinical results, emphasised by raised CD4-counts in laboratory tests, have been reported from Ethiopia (2002), Honduras (2003), India (2003), South Africa (2003), Malawi (2004), Nigeria (2005), Rwanda (2005), Central African Republic (2006), Cambodia (2007), Ghana (2007), Kenya (2007), Lesotho (2008), DR Congo (2009), Tanzania (2011), Uganda (2013). [1-5]
Comparative outcome study in rural AIDS clinics in Kenya (2017-2018)
Introduction: This research aimed at demonstrating that the immune system of HIV-positive patients can be enhanced using PC1.
Method: This was a naturalistic, non-randomised study with three comparisons: group 1 using only anti-retroviral drugs (ARVs) (n=99), group 2 using ARVs+PC1 (n=81) and group 3 using only PC1 (n=88). Patients were followed up for six months. Dependent blood sample-based variables were CD4-count and viral load. Dependent clinical variables were appetite, weight gain/loss, fatigue and weakness.
Results: A robust analysis was done on all variables, computing the differences between the baseline and the data from the last follow-up. A non-parametric statistical analysis showed that changes in all the variables are highly significant. The PC1-only group always had the best outcomes, the PC1+ARVs group second best, and ARVs-only group was always worst performing of the three groups. (Graph 1-2)
Summary: Evidence was found that PC1 effectively restores health in HIV-positive patients in Africa within a few months and prevents patients from relapsing with continuing treatment. It shows that the immune system can be restored and enhanced by using PC1. It also suggests that PC1 reduces the viral load. This first epidemiological comparative study shows that PC1 is a feasible treatment that can either be given alone or combined with ARV therapy in African HIV/AIDS patients and might thus be an inexpensive and safe therapy. Further work with longer periods of follow-up and randomised comparisons is needed to clarify the robustness of this finding. [15]
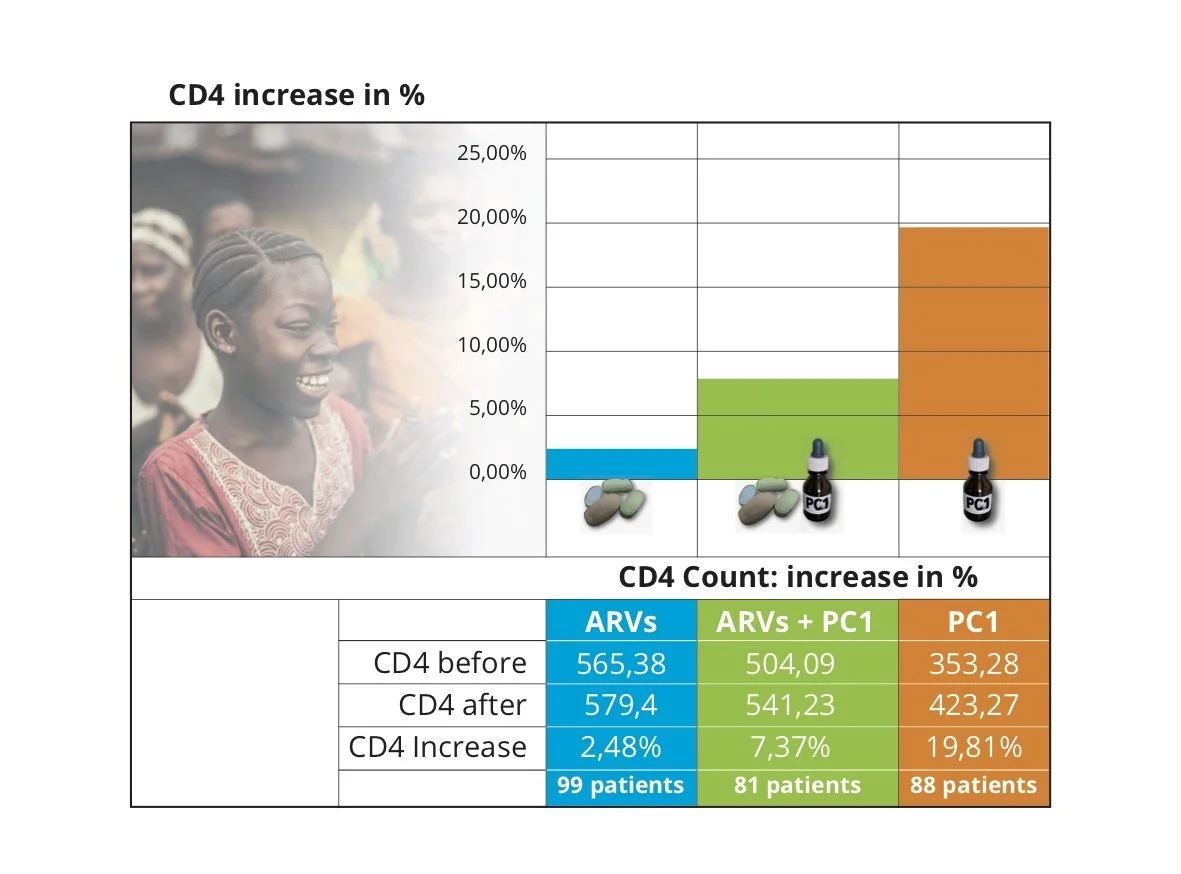
Graph 1: Percentage of increase of CD4-count after six months treatment in cells/m3
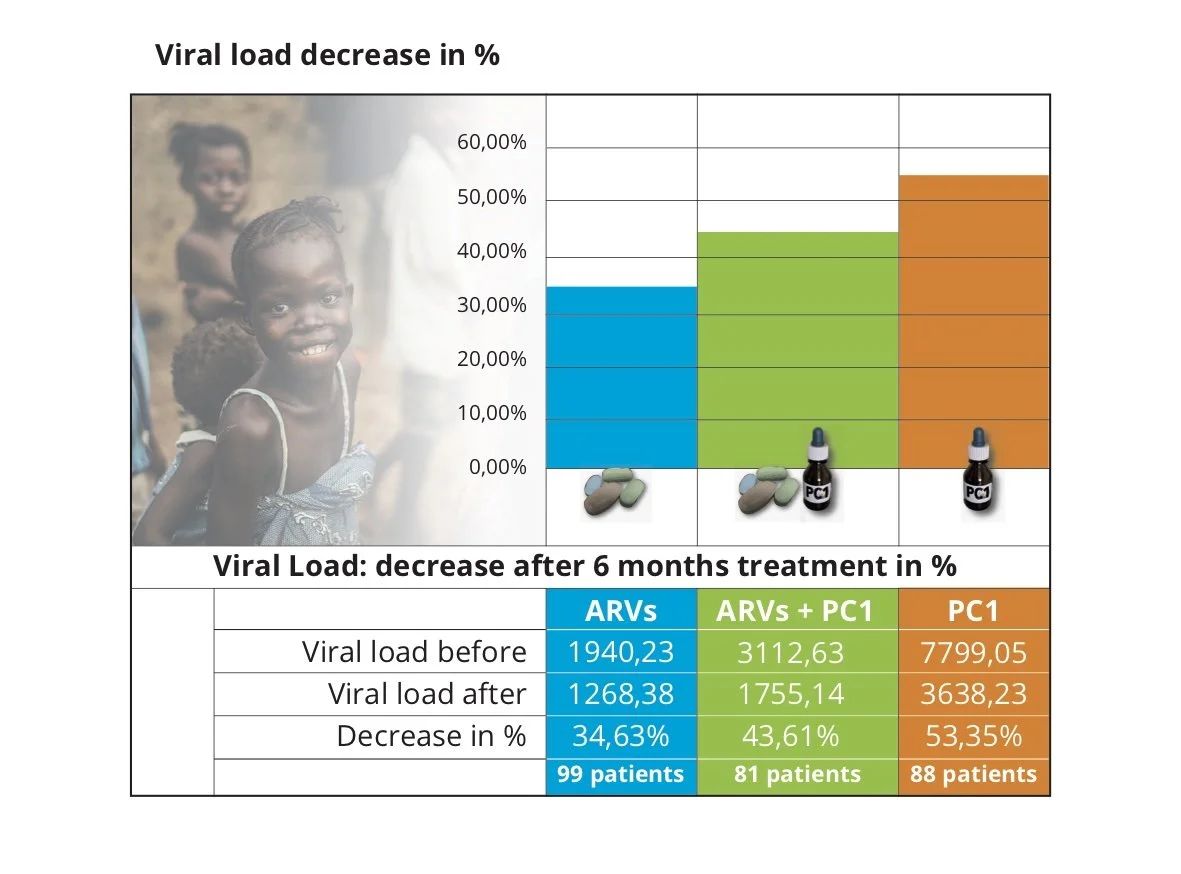
Graph 2: Percentage of decrease of viral load after six months treatment in copies/ml (viral units per ml. blood)
Malaria
Malaria is the main epidemic disease that causes death, disease and underperformance in Africa. While a milder form of malaria impaired the wellbeing of Europeans for centuries and could be eliminated, still, the much more severe tropical form poses the greatest threat to the health and wellbeing of people living in sub-Saharan Africa. In addition to causing immense suffering and numerous deaths, malaria hinders Africa’s progress and its potential to build a better future for its children. Utilizing resonance to prevent malaria and treat its chronic effects is a primary objective of ARHF.
Malaria predominantly affects children, as adults who have survived the disease in childhood generally develop sufficient immunological resistance. Despite the availability of regular medication and preventive measures, malaria remains a leading cause of death among African children. It is both a child killer and a disabler, severely affecting the health and development of young populations. Though data on malaria prevalence in Africa vary and are often based on estimates, they consistently reveal the vast impact this epidemic has on life in sub-Saharan Africa:
100-450 million clinical cases of malaria each year (WHO)
Approximately 400-600 thousand fatal cases of malaria each year (WHO)
Every minute an African child dies of malaria
1 out of 6 African children does not grow older than 5
In addition to malnutrition, malaria is a major cause of the fact that half of all African children are anaemic
Every school day up to 10-30% of children can be absent due to malaria
The cost of malaria to the economy in Africa is estimated at $12 billion annually.
For a long time medicine has been searching for an effective and sustainable way to treat and even prevent malaria, as this would greatly improve the quality of life in Africa. That way is available.
PC Malaria
The PC Resonance for malaria, called PC240m and produced by three European homeopathic pharmacies, has been used in Africa in thousands of cases ever since Peter Chappell first prepared it in 2002. This remedy has proved to be effective in treating acute malaria and chronic malaria as well as the long-term effects of malaria, for example, epilepsy or chronic headache occurring after having survived cerebral malaria.
What are the advantages of PC Malaria?
Very effective even in patients who do not respond to regular drugs
No side effects
Safe for infants, pregnant women and the elderly
Low cost
Production, distribution and storage are easy
No therapy resistance
With only a short training, every health professional can effectively prescribe it.
And there is still another huge advantage:
A resonance that heals a contagious disease may also help to build up resistance to that disease.
This means that PC240m can also be used to prevent malaria.
Africa Malaria Prevention Project
The ground-breaking observation, that treating malaria with PC240m also prevents the disease, led to the Africa Malaria Prevention Project (AMPP), which provides essential malaria prevention services to hundreds of thousands of children and adults through the available infrastructure of schools, churches, clinics, and village outreach programmes. [15]
Since its inception in Malawi in 2013, AMPP has demonstrated clear effectiveness. Significant reductions in school absenteeism, hospitalizations, and malaria-related deaths have been observed across various sub-Saharan countries.
Malaria research
Data collected from multiple schools highlights the impact of AMPP. Comparisons of absenteeism rates and school exam results before and after the implementation of AMPP show a dramatic decrease in absenteeism and, with the disabling condition almost absent, a significant improvement in academic performance. (See graph 3 for an example from a school in Kenya – 2014-2015.)
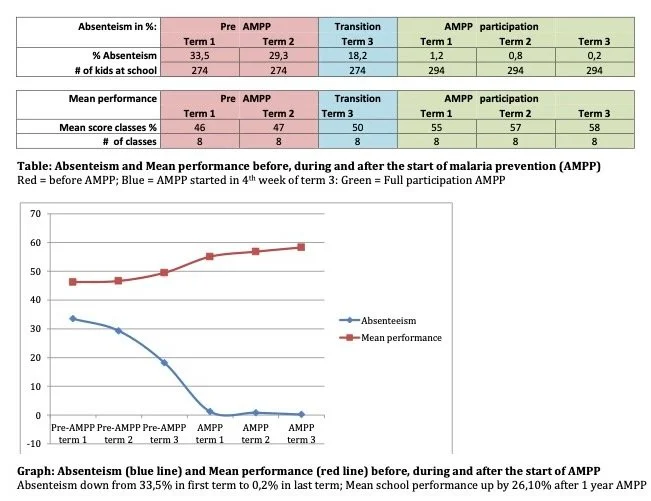
Graph 3: Absenteeism and Mean performance at a school in Kenya
In Malawi (2004) it was observed that the PC Remedy for treating malaria (PC240m) appeared to have an effect beyond curing acute malaria. Following treatment patients stayed free from frequent attacks for a period of six months or longer. This observation opened the possibility for testing out whether PC240m could be used for preventing malaria.
The first time this was observed was in DR Congo (2009). At a school in South Kivu, 600 children were given regular doses of PC Malaria. Within a few months, the school reported that no more cases of malaria had been observed. In a small Congolese town, PC Malaria was dispensed in the community by a church dispensary. Soon after, the local Red Cross hospital was seeing 95% fewer malaria cases, which even caused a new, unexpected problem: due to a lack of patients and thus income, they now had difficulty paying their nurses.
In Malawi (2012) a nursery that took care of 300 children lost five children each year because of malaria. The year they started giving PC240m to all children, they did not lose a single child.
Based on these results, the Africa Malaria Prevention Project (AMPP) was initiated, first in Malawi (2013). After offering AMPP to 27,000 people, schools reported reduced absenteeism while the local hospital observed reduced hospitalization and deaths from malaria.
In Kenya (2014) 5,000 school children received PC Malaria as prevention. In all participating schools absenteeism went down dramatically – by 80% or more. As increased school attendance might help to increase learning performance, the results of the state school exams were gathered from the year before and after AMPP. (See graph 4)
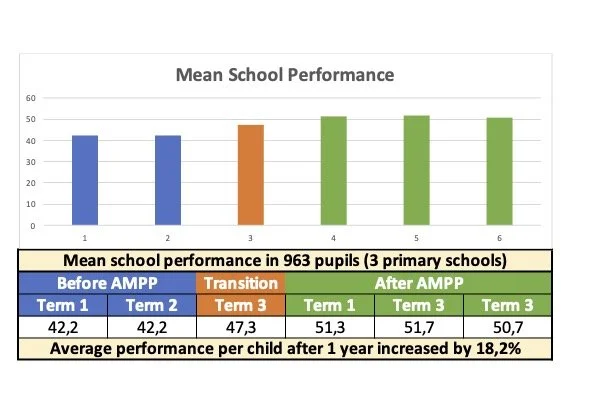
Graph 4: Mean school performance in 963 pupils (3 primary schools)
A Community Health Worker (Kenya 2014) formed a team of volunteers and made PC240m available to all 20,000 people living in and around her community, which used to have three to four funerals per week because of malaria or AIDS. Once PC Malaria was made available to the whole population, the local clinic confirmed that for more than six months nobody died from malaria. Here again the shift in health had an unexpected impact: The carpenter who had previously made three to four coffins a week shared the same information, changed his profession and became a priest. [15]
Epidemiological outcomes study in Bukavu, DR Congo (2018-2023)
Data from a six-year study conducted in Bukavu, DR Congo, demonstrates the impact of AMPP on malaria incidence and mortality. The part of the city where AMPP was available experienced significantly fewer malaria-related hospitalisations and deaths.
In 2023, AMPP was administered to 73,757 people, resulting in 4,162 fewer malaria cases than expected and 136 fewer malaria-related deaths, including 98 children under the age of five (a decrease of 80%).
An article on this study will be published in 2025. Here is a summary:
Introduction: This research aimed at demonstrating that the immune system of African people can be enhanced to prevent malaria by using PC240m. The Kadutu Commune where the study was performed consists of 13 health areas. To HA 1-5 PC240m was made available; HA6-10 served as cross over; in HA 11-13 PC240m was not made available.
Method: This was a non-randomised outcome study with health areas where AMPP was not made available for comparison. It was a naturalistic field study with the primary aim of serving people. Data from the year 2018, in which AMPP had not been started in any health zone, was used as a baseline.
Results:
Malaria related hospitalisation (see graph 5)
HA (Health Area) 1-5; population in 2019 resp. 2023, 180.464 resp. 208.453 (AMPP from 2019-2023): In 2022 resp. 2023 malaria cases had decreased by 36% resp. 30% compared to 2018. [In 2022 35% of the population in these HAs received AMPP, in 2023 19%; a reduced percentage as in 2023 the focus was on the new HAs.]
HA 6-10; population in 2019 resp. 2023, 145.700 resp. 162.190 (non-AMPP from 2019-2022; AMPP in 2023): In 2022 malaria cases had increased by 17% compared to 2018. After introducing AMPP in 2023, malaria cases had decreased by 37% compared to 2022. [in 2023 21% of the population in these HAs received AMPP]
HA 11-13; population in 2019 resp. 2023, 55.459 resp. 61.864 (non-AMPP from 2019-2023). Compared to 2018 malaria cases had increased by 33% in 2022 and decreased by 10% in 2023.
Malaria-related deaths (see graph 5)
HA 1-5 (AMPP from 2019-2023): In 2022 resp. 2023 malaria-related deaths had decreased by 72% resp. 79% compared to 2018.
HA 6-10 (non-AMPP from 2019-2022; AMPP in 2023): In 2022 malaria-related deaths had increased by 12% compared to 2018. After introducing AMPP in 2023, malaria-related deaths had decreased by 30% compared to 2022.
HA 11-13 (non-AMPP from 2019-2023). In 2022 resp. 2023 malaria-related deaths had decreased by 0% resp. 17% compared to 2018.
Summary: the data strongly suggest that PC240m can increase immunity against malaria and reduce malaria-related hospitalisations and deaths. In 2022, with 35% of the population in HAs 1-5 included in AMPP, a 36% reduction of malaria cases was seen, and 72% of malaria-related deaths. Further studies are recommended to observe the outcome when the full population of a certain area receive PC240m.
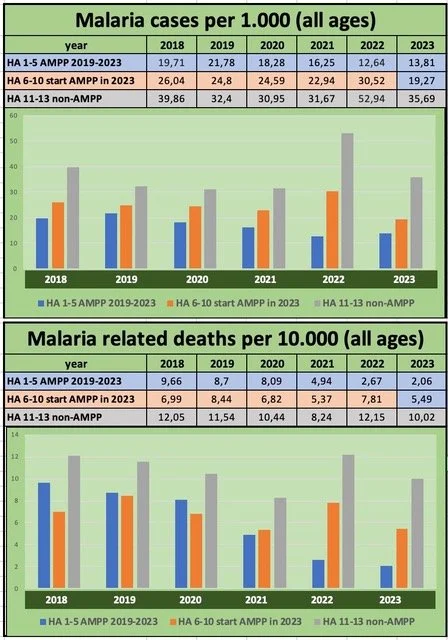
Graph 5: Malaria-related cases and deaths in 13 health areas in Bukavu (DRC) 2018-2023
The impact of the Africa Malaria Prevention Project
The following summarizes it most potently:

A child in the Malaria Prevention Project Malawi (Photo by Ruthee Sea Scoter, Malawi 2013)
It costs less than 10 cents per year to protect a child against malaria!
The Amma4Africa teams aim to reach 5-15% more people with AMPP each year. In 2024, they have already reached over 1 million children and adults, primarily in remote regions with little access to health care, but this is still only a fraction of the population in sub-Saharan Africa.
While the primary aim of ARHF is to alleviate suffering, it is also crucial to consider the socio-economic implications, as healthcare costs significantly affect the economy in Africa. The study conducted in Bukavu demonstrates that for every dollar spent on AMPP, the Social Return on Investment (SROI) in terms of the costs of health care can reach as high as 40 dollars.
See also the documentary “A message of Hope & Love”
Trauma relief
In recent years, war and natural disasters have brought home to us the lasting impact of psychological trauma on everyone’s wellbeing. Although Africa is often under-reported in the media in this regard, trauma has a significant impact on the health of African people. Since 2005, Peter has developed resonances for specific types of trauma, including those resulting from: war, genocide, rape, and natural catastrophes. Fast experience in using them has shown that the genus epidemicus approach can also be reliably used for collective trauma. PC Trauma resonances have been successfully utilized in thousands of cases, including in refugee camps and regions affected by natural disasters such as tsunamis and earthquakes. [15]
ARHF has developed an effective protocol for rapidly reaching as many people as possible following a traumatic event that involves thousands of people.
Aid workers, counsellors and therapists interested in using PC trauma resonances for treating individual or collective forms of trauma can contact ARHF to receive the free ‘ARHF Volunteers Manual – Basic Guide to Treating Infectious Diseases, Trauma & Chronic Diseases.’
At www.ARHF.nl an article on Treating Trauma in Refugees by Gunhild Quante (Germany 2018) can be downloaded.
See also the following videos: https://arhf.nl/en/videos
Rape Trauma – on the trauma of rape by rebels and soldiers in DR Congo
Rebels that got back to their senses – on rebels that decide to stop fighting after being treated for the trauma they themselves experienced
Nyarugusu Trauma Relief – on trauma relief inside a Tanzanian refugee camp
Haiti Trauma Relief 2010 – on trauma relief after the devastating 2010 earthquake in Haiti.
LEAP – Learning Enhancement Africa Program
‘Education is the most powerful weapon which you can use to change the world.’ – Nelson Mandela
LEAP is, in my opinion, the most revolutionary, ground-breaking and transformative development that Peter gifted to Africa.
To fully enjoy the benefits of education a child needs to be healthy, free from stress and possess good learning skills. LEAP is designed to support a child on all these levels. Beyond intellectual learning, LEAP is therefore also about the body-mind learning how to deal with infectious agents and how to process trauma.
Besides water, sound can also be imprinted with coherence inducing information to enhance health and wellbeing. Sound is an ideal medium for schools, where large numbers of children are gathered. Using audio has many practical advantages:
Instead of giving each child an oral dose of a remedy, all can listen to the same sound.
Ideally one only imprints water with information related to one condition, as otherwise all the data gets mixed up. However, as a sound file has a duration in time, a lot of information can be embedded in sequential order.
Contents of LEAP
The actual contents of LEAP are imprinted in a piece of music but are itself not audible. They concern:
Prevention and treatment of all relevant infectious diseases in Africa and their short- and long-term consequences: HIV, parasitic worms, malaria, typhoid, tuberculosis, ringworm, scabies, diarrhoea, syphilis, gonorrhoea and lower respiratory tract infections (RTIs)
Releasing and evolving through all the effects of past traumas: injury, bereavement, war and genocide, shock, orphan trauma, rape trauma and inappropriate triggers to freeze, flight and fight survival instincts
Enhancing and resolving all impediments to learning skills: awareness, intelligence, creativity, grounding, centring and stillness, numeracy and literacy ability, concentration and focus.
LEAP-Protocol for schools
It is recommended to play LEAP at the start of each school day. Depending on how loud is possible, it can be played to each class separately or to all children gathered together.
It is recommended that children relax and keep quiet during listening. It may be helpful to keep the eyes closed.
Teachers should observe:
• Better attendance due to better health,
• Better attention and openness in class, higher marks and
• Signs of all-round improvement in learning.
First feedback
LEAP was first tested out in several schools in Kenya. Data regarding absenteeism and learning performance were gathered from before and after LEAP. The results were very encouraging. Heads of schools reported:
Significantly improved absenteeism (up to 80% less)
Reduced hospital reference for children falling sick during classes
Children with epilepsy, caused by birth trauma or cerebral malaria, had significantly fewer attacks
Reduced stress levels and fewer behavioural problems
Improved school performance in end-of-term tests.
See the videos LEAP Kenya 2015 evaluation and Africa Malaria Prevention and Learning Enhancement Project for an impression of the impact headmasters reported.
What was very touching is that all headteachers of LEAP-schools that were interviewed spontaneously reported that the relationship between children and teachers had improved a lot, so much so that the cane had now become a relic of the past. Just beautiful!
LEAP data collection
The impact of LEAP on absenteeism and school performance is remarkable. After using LEAP for one year in 16 schools, average absenteeism decreased by 65% compared to the previous year (see graph 6).
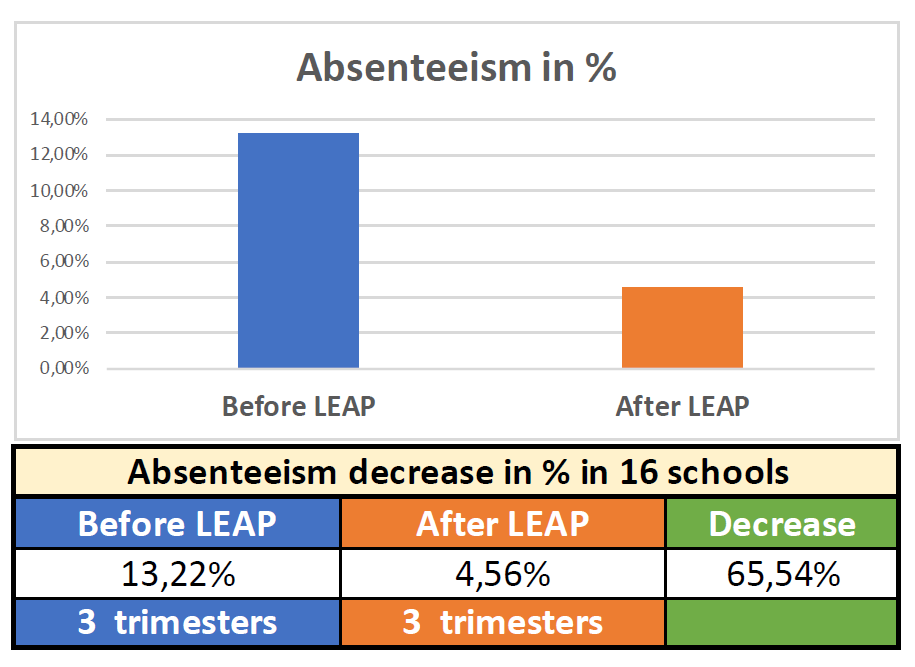
Graph 6: decrease of absenteeism as a result of LEAP
One of the first schools adopting LEAP was Marega Primary School. After a full year of using LEAP the mean school performance measured through state examinations had increased by 26%. After four years of using LEAP the school scored second best of all primary schools in Kenya – an extraordinary result for a school with minimal means, situated in a poor rural area that is regularly hit by excess rains and floods.

Photo: Marega Primary School
These data show that LEAP is literally helping children to have a healthy and bright future. LEAP can easily be rolled out all over Africa. All a school needs is a simple MP3 player or speaker (found all over Africa for $15-25) and a USB-stick. See below for the simple LEAP-protocol.
The advantages for children and their parents are:
Better health and less sickness
Reduced healthcare expenses as hospitalisations reduce
Improved results at primary school allowing children to move on to secondary school, with better chances for pursuing their dreams and using their talents.
Further development of LEAP
A LEAP-app will be created, making it possible for users to play LEAP from a smart phone. This also means that schools that cannot be reached by our extensive network of volunteers can obtain and use LEAP.
LEAP for all ages
LEAP was originally designed for school children, but to be free from infectious diseases, stress and trauma, and to have good functioning mental faculties is important at all ages. LEAP can therefore be used by and for anyone. The availability of LEAP in the form of an app, which is to be developed soon, will make it possible for anyone with a smartphone to download it for free.
Sickle cell anaemia
Sickle cell disease (SCD) is a genetic lifespan-reducing and disabling condition common in Africa and challenging to treat. As there is no cure, conventional treatments have focused on managing symptoms and preventing complications, but even these options are often unavailable or insufficient in African settings.
In 2013, PC1436n for treating SCD has been introduced and suggested for treatment in several sub-Saharan countries. An article published in 2018 concludes that PC1436n offers a cost-effective and accessible alternative that has shown significant improvements in the lives of SCD patients across various age groups, and calls for further research, training, and dissemination of this treatment approach to reach more individuals affected by SCD. [23] (see graph 7).
ARHF is planning an observational, prospective cohort study, to be conducted across multiple African healthcare centres over a period of 24 months. Patients with SCD who are prescribed PC1436n as part of routine clinical care will be enrolled in the study, which is expected to start in 2025. The study has the following objectives:
To assess the real-world effectiveness of PC1436n in reducing the frequency and severity of vaso-occlusive crises in patients with SCD
To evaluate the impact of PC1436n on healthcare resource utilisation, including hospitalisations and emergency department visits
To evaluate the impact of PC1436n on complete blood count and haemoglobin levels
To explore patient-reported outcomes such as pain intensity, quality of life, and overall treatment satisfaction.
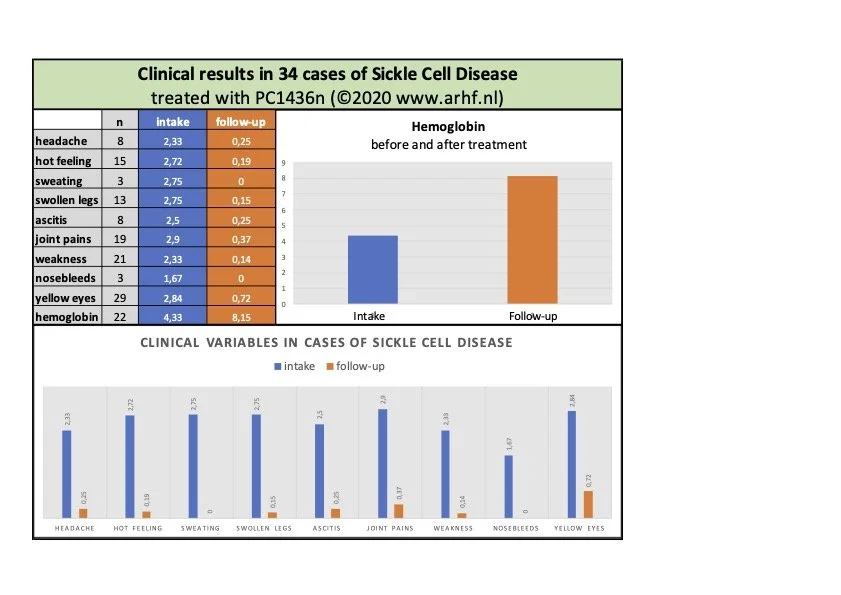
Graph 7: Clinical results in 34 cases of sickle cell anaemia
Social return on investment (SROI)
To put a price tag on human lives feels unnatural but nevertheless, for many stakeholders, and especially larger donors and authorities, knowing the monetary effectiveness of an investment in health programmes weighs strongly in their decision-making. Therefore an SROI-analysis was made for the Malaria Prevention study performed in Bukavu.
Social return on investment analysis for 2023 malaria prevention in Bukavu (DRC) – SROI analysis for a population of 370,634 in Kadutu health zones 1-10
The investment for making PC240m for malaria prevention available to 73,757 in 10 health zones in Kadutu district was $4,300.
The data of 2023 were compared with 2018 figures when PC240m was not used in Bukavu. The population of health zones 11-13, where PC240m was not used, served as the control group. Data were adjusted for population changes in each area.
Outcomes:
For children aged 0-5:
273 fewer treated as outpatients for malaria
950 fewer hospitalised for malaria.
For individuals aged 6 and older:
105 more treated as outpatients for malaria
3,044 fewer hospitalised for malaria.
Malaria-related deaths reduced:
98 fewer deaths among children aged 0-5
38 fewer deaths among individuals aged 6 and older.
Impact:
Improved overall health of the population
Reduced malaria-related treatments and deaths
Decreased absenteeism from school or work
Reduced socio-economic losses.
Monetary valuation:
Outpatient treatment costs for children aged 0-5: $10 each
Savings: 273 x $10 = $2,730
Hospitalisation costs for children aged 0-5: $35 each
Savings: 950 x $35 = $33,250
Treatment costs for individuals aged 6 and older: $14 on average
Additional cost: 105 x $14 = $1,470
Hospitalisation costs for individuals aged 6 and older: $45 on average
Savings: 3,044 x $45 = $136,980
Economic loss (lost future earnings + parental work loss) for children aged 1-5: $23,000 each
Savings: 98 x $23,000 = $2,254,000
Economic loss for individuals aged 6 and older: $19,600 each
Savings: 38 x $19,600 = $744,800.
Social return on investment (SROI):
Healthcare savings:
Outpatient treatment savings for children aged 0-5: $2,730
Hospitalisation savings for children aged 0-5: $33,250
Additional outpatient treatment costs for individuals aged 6 and older: -$1,470
Hospitalisation savings for individuals aged 6 and older: $136,980
Total health care savings: $171,490.
Economic Loss savings:
Savings from reduced deaths among children aged 1-5: $2,254,000
Savings from reduced deaths among individuals aged 6 and older: $744,800
Total economic loss savings: $2,998,800.
Total social value created:
Health care savings: $171,490
Economic loss savings: $2,998,800
Total: $3,170,290.
SROI calculations:
Health care savings only:
$171,490 / $4,300 = 39.88
Health care savings + economic loss:
$3,170,290 / $4,300 = 737.27.
Summary: The SROI analysis for the malaria prevention programme in Bukavu shows a significant return on investment, especially when considering broader socio-economic impacts. The high SROI suggests that expanding the programme to more health zones or regions with high malaria prevalence is highly recommended.
Conclusion
The Amma Resonance Healing Foundation (ARHF) and its initiatives exemplify a commitment to alleviating suffering and fostering health through innovative methods founded on the principles of homeopathy. Based on the amazing legacy of Peter Chappell, the ARHF has made remarkable strides in addressing critical health challenges such as HIV/AIDS, malaria, and trauma across sub-Saharan Africa. Its evidence-based, scalable approaches demonstrate the transformative potential of PC Technology and LEAP programmes in improving health outcomes, empowering communities, and enhancing education.
These achievements are only possible through collective effort. We invite you to join this transformative journey. Support ARHF by contributing financially to sustain and expand these impactful projects or by actively volunteering to further its mission. Together, we can help ARHF reach even more underserved communities, ensuring health, dignity, and opportunity for all. Visit ARHF’s website https://arhf.ngo– to learn how you can make a difference today. Please contact us for any questions or suggestions you may have.
References
Henry M, Schwartz L. Entropy export as the driving force of evolution. Substantia 2021; 3(2):29–56. https://doi.org/10.13128/Substantia-324
Manzalini A, Galeazzi B. Explaining Homeopathy with Quantum Electrodynamics. Homeopathy 2019;108(3):169-176. doi: 10.1055/s-0039-1681037
Gerbaulet J, Henry M. The ‘Consciousness-Brain’ relationship. Substantia 2019; 3(1):113-118. doi: 10.13128/Substantia-161
Madl P, Renati P. Quantum Electrodynamics Coherence and Hormesis: Foundations of Quantum Biology. Int J Mol Sci. 2023 Sep 12;24(18):14003. doi: 10.3390/ijms241814003.
Shiah YJ, Shan L, Radin DI, & Huang GT. Effects of Intentionally Treated Water on the Growth of Mesenchymal Stem Cells: An Exploratory Study. Explore 2021, S1550-8307(21)00242-1. https://doi.org/10.1016/j.explore.2021.11.007
Henry M. Consciousness, Information, Electromagnetism and Water. Substantia 2020;4(1):23–36. doi: https://doi.org/10.13128/Substantia-645
Al-Khalili J, McFadden J. Life on the Edge: The Coming of Age of Quantum Biology. Broadway Books; 2015.
Chappell PL, The Successful Homeopathic Treatment of HIV/AIDS – An Appeal for Help, Homœopathic Links, Vol 15:4, 2002
Hiwat CM, van der Zee HE, PC1 – An Answer to AIDS in Africa, Homœopathic Links, Vol 17:4, 2004
Schustereder K. PC 1 als homöopathische Arznei bei AIDS: Erfahrungen aus der staatlichen Klinik Baboua in Zentralafrika. AHZ 2007;252(3):109-118
Chappell PL, The Second Simillimum, Homeolinks Publishers, Haren (Netherlands) 2005
Chappell PL, van der Zee HE, Homeopathy for Diseases, Homeolinks Publishers, Haren (Netherlands) 2012
Van der Zee HE. Africa Malaria Prevention Project. Homoeopathic Links 2016;29(2):137–146.
Van der Zee HE et al. Treating Sickle Cell Disease in Africa. Homoeopathic Links 2018;31(2):120–126
Van der Zee HE, Wallach H. Novel Immune Supportive Treatment of HIV/AIDS – Comparative outcomes study in rural clinics in Africa. The International Journal of Healing and Caring. 2024, 24(1) 18-34. https://doi.10.78717/ijhc.2024118
Pollack GH. The Fourth Phase of Water: Beyond Solid, Liquid, and Vapor – unveiling the secrets of the world's most common substance. Ebner and Sons Publishers. 2013.
Gerbaulet J, Henry M. The ‘Consciousness-Brain’ relationship. Substantia 2019; 3(1):113-118. doi: 10.13128/Substantia-161
Emoto M. The secret life of water. Atria Books. 2011
Austin V. The Secret Intelligence of Water: Macroscopic Evidence of Water Responding to Human Consciousness. Lifestyle Entrepreneurs Press. 2021
Henry M, Schwartz L. Entropy export as the driving force of evolution. Substantia 2021; 3(2):29–56. https://doi.org/10.13128/Substantia-324
van der Zee HE. Healing Humanity with Homeopathy: Homeopathy for Epidemics, Collective Trauma and Endemic Diseases. Wholistic Healing Publications 2009;9(2)
van der Zee HE. ARHF Volunteers Manual 3.0: Basic Guide to Treating Infectious Diseases, Trauma and Chronic Diseases. Amma Resonance healing Foundation: Haren, Netherlands; 2022.
Achieng B, Omondi M, Balikwisha N, Hongo Y, Akpabio E, Chappell P, Van der Zee H. Treating Sickle Cell Disease in Africa. Homoeopathic Links 2018;31(2):120–126
Harry van der Zee
Harry van der Zee (b. 1953, Netherlands) is a homeopathic doctor since 1987. He served as editor-in-chief of Homœopathic Links (1996–2018) and has lectured globally on homeopathy. His work emphasizes the birth experience's role in understanding miasms, explored in his books Miasms in Labour (2000) and Homeopathy for Birth Trauma (2007).
Since 2004, he has focused on healthcare in Africa and derangements of the vital force within the collective. Co-founding ARHF in 2007, he trained health workers to treat and prevent epidemics, trauma and chronic diseases with PC Resonances. With Peter Chappell he co-authored Homeopathy for Diseases (2012) and produced documentaries on conditions like AIDS and malaria. Harry has published research on HIV/AIDS and malaria prevention and currently focuses on conducting studies on sickle cell disease treatment. His efforts, including organizing the 2009 Homeopathy for Developing Countries conference, aim to integrate homeopathy and its principles into global healthcare solutions.
This article was first published in the UK journal: Homeopathy in Practice Journal of the Alliance of Registered Homeopaths UK.